Medication complexity is a challenge to patients, physicians, and pharmacists alike. It occurs when an individual is prescribed multiple medications, each with its own dosing schedules and side effects, without sufficient support and guidance. In particular, people with complex health and social needs are often juggling medications with no single entity coordinating the overall medication regimen to ensure that these medications as a whole will not lead to worse health, hospitalizations, or even premature death. Despite these challenges, there is typically limited attention paid to the issue.
Jim Slater, PharmD, executive director of pharmacy at CareOregon — a coordinated care organization that primarily serves Medicaid and Medicare special needs populations — is at the forefront of defining and understanding the concept of “medication trauma.” This is how he refers to the many instances he sees when patients become overwhelmed by complicated drug regimens and experience fear, anger, anxiety and/or frustration, which can result not only in adverse drug events, but in trauma — physical or emotional — for the patients. The Center for Health Care Strategies recently spoke with Dr. Slater to discuss medication trauma, the innovative tools his team uses to identify patients at risk, and how other organizations can address this issue.
Q: You use the term “medication trauma” — what does that mean?
A: Medication trauma is a combination of medication complexity and the lack of coordination that overwhelms patients, caregivers, and providers. It can create fear, confusion, and error, which can lead to poor adherence and outcomes. As providers, we can sometimes reach a place in caring for a patient where, in trying to do a good thing in meeting their health needs with medications, gaps and barriers may occur, and instead of medications helping the person, they actually start to become a source of trauma.
Q: What was the impetus for CareOregon’s focus on medication trauma?
We kept hearing patients say they wanted help with their medications. As we unpacked what that help should look like, we realized how frustrated, fearful, and overwhelmed they were.
A: Six years ago we conducted listening sessions with providers to inform the expansion of our clinical model and uncovered a troubling cycle. Many of our patients with physical and behavioral health comorbidities (e.g., anxiety, depression, PTSD) were presenting in an activated state of trauma and were experiencing a worsening disease state. We found that in an attempt to stabilize patients, providers were adding more medications — often exacerbating the trauma. In tandem, our CEO recognized the power of listening to our members and partnered CareOregon with IDEO to teach us human-centered design. The model was clear: dispel everything we know, meet people ‘where they are at,’ and let them identify their own needs. When we did this, we kept hearing patients say they wanted help with their medications. As we unpacked what that help should look like, we realized how frustrated, fearful, and overwhelmed they were. Combining these two points of view — the health professionals and patients we serve — we had a fresh sense of what to focus on. This was the trigger to make us further dig into the space of medication trauma.
Q: What are the “aha” moments when addressing medication trauma?
A: A big one was that when a person is experiencing medication trauma, the way to deal with it is not necessarily to start by tracking down all their medicines and performing medication therapy management (MTM) and medication reconciliation, which is a very defined process you go through to tidy things up. The “aha” was when we found it was actually more powerful to connect with the patient and find out what matters to them now. That means waiting to address the health conditions with MTM, and instead work on building a relationship of trust so we can discern the patient’s most important goals from his or her perspective. We found a simple way to do this: create a list of the patient’s medications using our MEDS (My Easy Drug System) chart and ask him or her to talk about his or her emotions around each one by circling a corresponding face (happy, angry, or indifferent). This is an excellent way to triage what to focus on, build a rapport, and unravel medication trauma and care coordination issues. We celebrate the ones that the patient is happy about, and discuss the ones that are troubling. Then, we begin medication reconciliation.
Another big “aha” was learning that medication coordination is a very powerful way to go about our work. We have developed an algorithm, currently patent pending, which is an objective way to use pharmacy data to find the people most at risk for medication complexity, which turns out to be an excellent future predictor of emergency department and hospital use with only pharmacy claims.
Q: Would you tell us a little bit about the algorithm — how are people initially identified for medication complexity?
A: By using four to five pharmacy claims variables, such as the number of providers, pharmacies, and medications, and how often they are being filled, we get a very good prediction of future emergency department and hospitalizations. We only need 90 days of claims to run the algorithm, which then provides us with a risk score. The average score is a six. We have discerned that the sweet spot for medication complexity is around a nine. When a patient is flagged at a nine, we know they are at high-risk for medication complexity, which suggests we need to connect with him or her to ensure everything is okay from an emotional and clinical perspective.
Q: Do you have a compelling patient story that illustrates the need for programs focused on medication trauma?
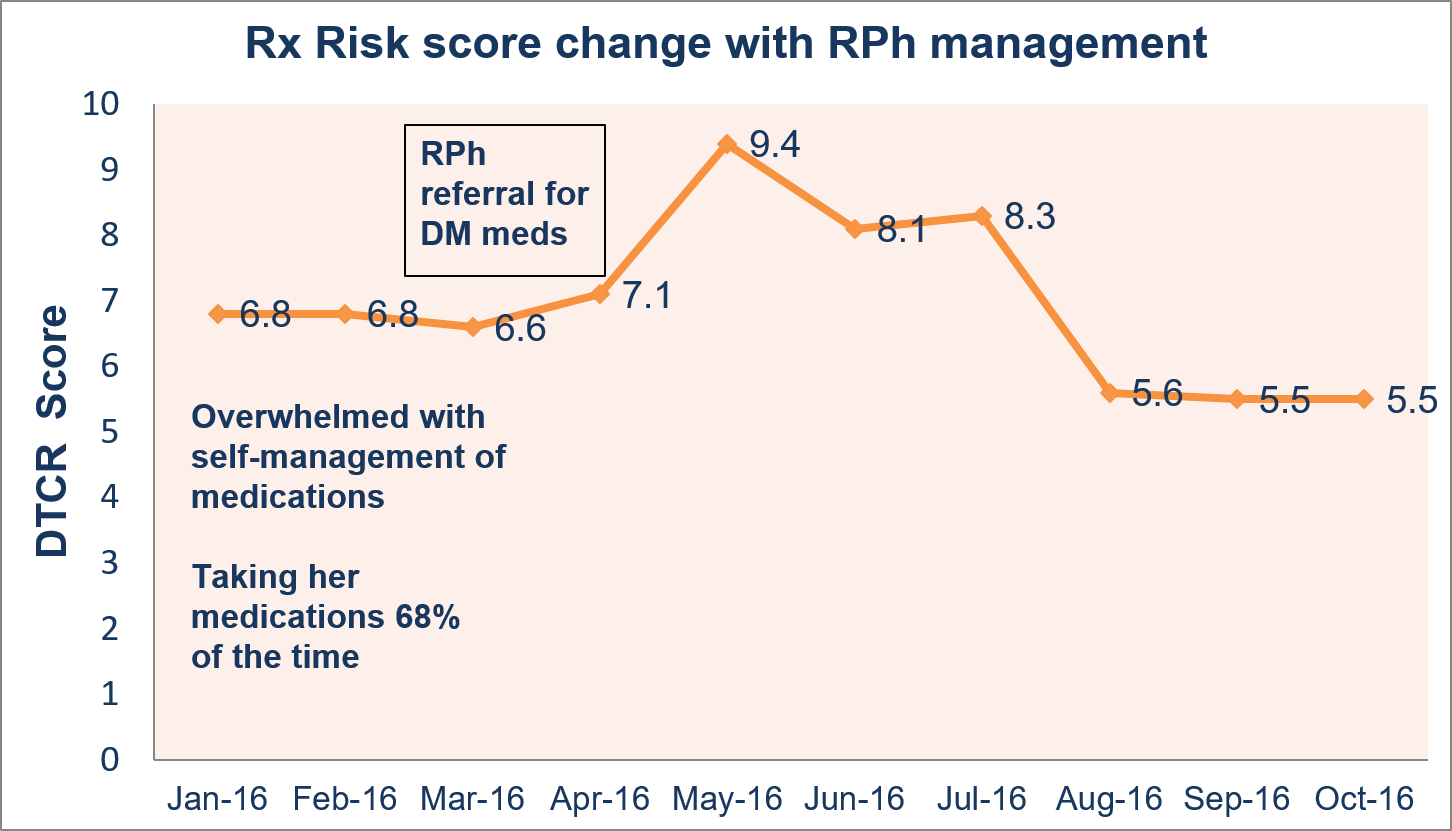
Medication coordination that correctly spots and intervenes on at-risk situations is a powerful tool to help patients.
A: We partner with Central City Concern, a clinic and pharmacy organized around the homeless population in Portland. They have used our pharmacy risk score algorithm and MEDS chart to find and help their patients in trouble. One of its patients had a normal risk score (6.6-6.8) for the first three months. In month four, it climbed to 7.1, then leapt to 9.4 in month five, triggering an assessment process. The pharmacist who received this patient’s case checked in with her and found that she was overwhelmed with her medications, and as a result was not taking them correctly and/or not taking them at all about two-thirds of the time. She had too many medications and had lost track of what to do when. After working with the pharmacist, the patient was empowered to take an active role in the self-management of her medications as well as better communicate when she was frustrated or confused. Her risk score dropped almost immediately to an 8.1 the following month, and two months later stabilized at a 5.6 — a better score than before she even triggered the system. This demonstrates that medication coordination that correctly spots and intervenes on at-risk situations is a powerful tool to help patients.
{kind=link}
Q: What is your advice to an organization that is interested in developing a similar model for complex populations?
A: Using a chart such as MEDS is an excellent way to find those one or two problem areas to begin working on with a patient. Patients tend to pick what is important clinically anyway, and it also empowers them to share their view. If you can allow that to occur and stay organized in tracking what you are learning with each patient, you can begin to study patterns, which opens you up to do PDSA cycles, training, and filling gaps of care with new services or relationships with provider partners. The pharmacy risk score is one nice way to do this because it is objective and only requires pharmacy claims. But above all, it is important to recognize the human element in this work — the time and trust required to build relationships, which is key to engaging a patient and preventing medication trauma from ever occurring.

For many of us who go through this type of trauma in childhood, it is chronic trauma & can destroy our entire life trajectory. There is a need for much more transparency in discussing the impact that this negligence has on patients. I fear that corporate healthcare will not allow for the form of honesty that is necessary for the damage to accurately be observed. Therefore it likely will not be fully addressed, which is unacceptable as it would lead to more trauma & death. Much more research must be done, as this seems to be a recent discovery. Understating… Read more »