At-A-Glance
ORGANIZATION: OneCare Vermont, an all-payer accountable care organization (ACO) serving roughly 250,000 Vermonters
INNOVATION: COVID-19 Care Coordination Tool
GOAL: Assist providers in reaching patients who have chronic conditions and behavioral health issues who might need immediate care and those who are at highest risk of poor outcomes from COVID-19.
KEY FEATURES:
• Identifies high-risk patients via an online data tool using specific criteria
• Provides a script for “care and concern” calls led by licensed or unlicensed staff
• Allows continuity of care while primary care practices are doing no or limited in-person visits due to COVID-19
Norm Ward, MD, a family practitioner and chief medical officer for OneCare Vermont, was concerned that he had seen very few patients in his office since COVID-19 stay-at-home orders were issued. Many of his patients were older and suffered with chronic conditions and he knew these individuals were at higher risk of getting sick or potentially dying from COVID-19 if they were infected. At the same time, patients with chronic needs were not seeking care due to the pandemic. Did they need care for medical issues besides COVID-19?
He had no way to systematically identify patients with specific high-risk factors through his electronic health record. “When you ask any clinician: ‘Who are your high-risk people?’ Even though doctors are proud to say, ‘I know all my patients really well,’ there’s just no way that you can remember everybody,” said Dr. Ward.
Like other primary care providers around the country, Dr. Ward and his staff were working remotely. Staff who normally did things like room patients, take vitals, and assess why a person had come in for a visit, found they had time, but had no roadmap for how to face the overwhelming task of trying to identify and reach their most at-risk patients.
Innovation | An Online Data Tool to Identify High-Risk Patients
“When you ask clinicians: ‘Who are your high-risk people?’ Even though doctors are proud to say, ‘I know all my patients really well,’ there’s just no way that you can remember everybody.”
To support practices like Dr. Ward’s, OneCare Vermont’s Analytics team created the COVID-19 Care Coordination Tool. The team is comprised of public health and analytics experts who leveraged publicly available risk criteria and combined that with the data and tools at OneCare. The tool combines medical and pharmacy claims information, as well as data indicating medical and social complexity, to create lists of high-risk patients and flags those at highest risk of a poor outcome if the individual were to contract COVID-19. Leveraging guidance from the Centers for Disease Control and Prevention, the World Health Organization, and Johns Hopkins, the self-service tool allows users to filter by risk criteria to prioritize outreach to patients (see exhibit below). It is available to OneCare participants via WorkBenchOne, OneCare’s informatics platform supported by Health Catalyst. Practices in OneCare can log into WorkBenchOne and narrow down their patient population by risk factors. They can export and share this list with practice staff who can use it to guide patient outreach calls.
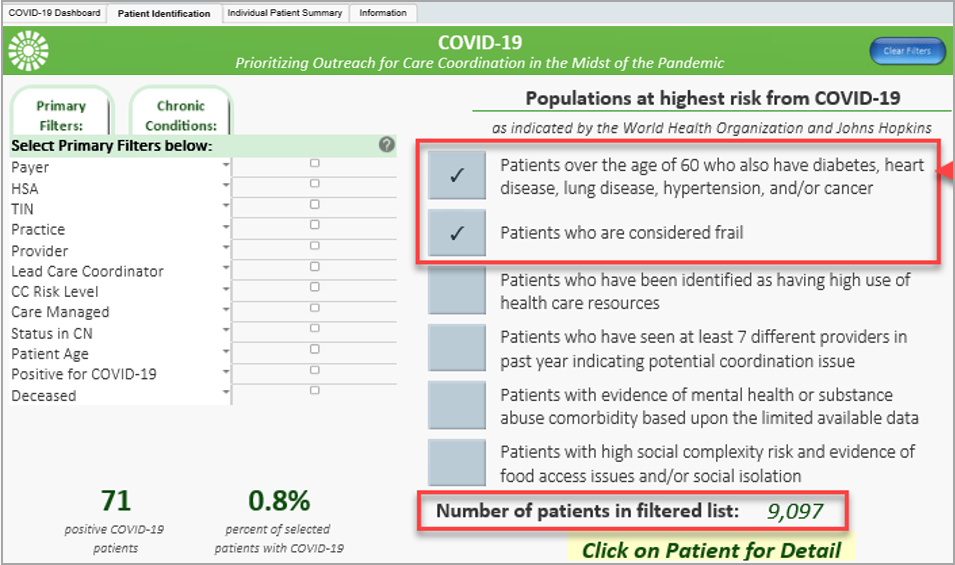
Exhibit. OneCare’s Care Coordination Tool in Action
This is a screenshot of OneCare’s care coordination tool in action — the user is filtering to identify frail older adults over the age of 60 who have chronic conditions.
Patients must meet one or more of six vulnerability criteria to be considered high risk:
| Risk Factor | Tool/Measure |
|---|---|
| Age greater than 60 with chronic conditions | Johns Hopkins ACG System* |
| Frailty score | Johns Hopkins ACG System |
| Patients who have seen at least seven different providers in past year, indicating a care coordination issue | Johns Hopkins ACG System |
| Mental health or substance abuse comorbidity | Johns Hopkins ACG System |
| High health care resource usage | Johns Hopkins ACG System |
High social complexity groups and evidence of:
| Food access issues:
|
* The Johns Hopkins ACG System accounts for demographics, medical claims, and pharmacy claims.
Implementation | Putting High-Risk Patient Lists to Work through “Care and Concern” Calls
“For those who live alone, feelings of isolation may be strong. Video or telephone visits are good ways to receive counseling and emotional support in place of in-person visits.”
With the patient list generated in OneCare’s COVID-19 application, Dr. Ward and his colleagues were able to proactively outreach to their high-risk patients. OneCare refers to these as “care and concern” calls, and provides an optional script for staff to use in practices. Practices conduct these outreach calls using licensed or unlicensed staff, determine potential care needs, and, if necessary, schedule follow-up telemedicine visits. The care and concern calls can target individuals at highest risk for poor outcomes due to COVID-19, but they may also serve as “pre-visit planning” for a virtual or telephonic visit for patients with chronic physical and behavioral health conditions.
“Through the calls, we were able to initiate clinical contact with individuals who may not have realized that they could present a non-COVID-19 type issue and continue their regular medical care,” said Dr. Ward. Because this tool aids providers in helping patients continue needed care, OneCare hopes it will decrease potential pent-up demand for services once the threat of COVID-19 lessens, allowing patients to safely return to primary care. Initial feedback from practices using this tool suggests they are catching patients with acute issues who were simply staying at home and many patients have been very appreciative for the outreach.
Future Lessons | Shifting the Focus of Patient Engagement and Care Delivery over the Long Term
“Practices that have been proactively reaching out to their high-risk patients may find that they have improved engagement of a traditionally hard-to-engage population and have built stronger relationships.”
“Staying home saves lives during the COVID-19 pandemic. Yet, many people have been home by themselves for months and may be feeling very isolated,” said Tyler Gauthier, director of value-based care at OneCare Vermont. “By receiving these calls patients know someone is ‘in this with them’ and they will have a contact person in case they have additional concerns. Over time, practices that have been proactively reaching out to their high-risk patients may find that they have improved engagement of a traditionally hard-to-engage population and have built stronger relationships.”
Having a list of high-risk patients also gave Dr. Ward and his staff a clear way to organize remote care delivery. It encouraged his practice to use a population approach to care, something they had been wanting to adopt prior to COVID-19, but had trouble instituting when they were busy seeing patients. “At OneCare, we have been working to promote care coordination payments for coordinating services for the high- and very high-risk,” said Dr. Ward. “This tool helps staff understand and practice what a population health approach to care looks like.”
To date, 30 organizations in OneCare’s network are using the care coordination tool independently to identify high-risk patients who may need tailored outreach during COVID-19 stay-at-home orders. Other organizations that are not using the tool are benefiting from OneCare’s outreach and are being provided a list of high-risk patients securely. Moving forward, OneCare is seeking to standardize this tool and care process to deliver better care for those at high risk even after the COVID-19 pandemic.
Additional Resources
COVID-19 Workflow and Script for High Risk Patient Outreach – OneCare’s recommended workflow to assist organizations in conducting high-risk patient outreach, and its “care and concern” call script.
COVID-19 Care Coordination Prioritization Application Handout – OneCare flyer used to promote its care coordination data tool to provider practices with information on how to access and use the tool.
About the Center for Health Care Strategies
The Center for Health Care Strategies (CHCS) is a nonprofit policy center dedicated to improving the health of low-income Americans. It works with state and federal agencies, health plans, providers, and community-based organizations to develop innovative programs that better serve people with complex and high-cost health care needs. OneCare Vermont is a pilot site in CHCS’ Advancing Integrated Models initiative, a national multi-site demonstration assisting health systems and community providers in integrating innovative, person-centered approaches for individuals with complex health and social needs
Authors: Karla Silverman and Emma Opthof, Center for Health Care Strategies.
